Aim: To evaluate the accuracy of intaglio surface
of complete dentures fabricated by additive and
subtractive manufacturing methods.
Settings and Design: This was a systematic review
and meta-analysis following the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses
(PRISMA) guidelines.
Methods and Material: An electronic search of
PubMed (including MEDLINE), EBSCO host databases,
Cochrane library and Google Scholar search engine
for articles published from January 2011 to Feb 2023
was conducted. The literature search intended to
retrieve all relevant clinical and in vitro studies about
the accuracy of the intaglio surfaces of the complete
dentures fabricated by additive and subtractive
manufacturing methods.
Statistical analysis used: Meta-analysis was
conducted in from the reported quantitative data.
Results: A total of 1468 articles were obtained via electronic search; 10 studies met the inclusion
criteria and were included in this systematic review
out of which 8 were in vitro studies and 2 were
clinical trials. Among the different parameters
described, the accuracy of the intaglio surfaces
of the complete dentures fabricated by different
manufacturing methods were evaluated. Accuracy
was measured by superimposition technique. 8
studies which evaluated the accuracy of the
dentures were included in meta-analysis.
Accuracy between the intaglio surfaces of dentures
showed a statistically significant difference between
milled and 3D printed complete dentures (P < 0.05,
pooled mean difference ranging from -0.13 to 0.18)
Conclusions: There is an overall increased accuracy
in the intaglio surface of the milled complete
dentures when compared to the 3D printed dentures,
thereby making them more preferred.
Key words: Accuracy, complete dentures, CAD CAM, additive manufacturing, subtractive manufacturing
Edentulism can reduce the quality of life
associated with dental health by affecting
appearance, phonation, and function that
can be restored by placing new removable
dentures.1,2 There are numerous techniques by
which a complete denture can be fabricated and
the purposes of each technique are to provide
prosthesis with ultimate mucosal adaptability
and reduce processing error resulting in
good retention, support, and stability. The
clinical protocols involved in the production
of a conventional complete denture may be
complicated, time-consuming, and difficult to
control quality from the laboratory process.3
The adaptation of a removable complete denture
to the underlying soft tissues is important for
retention, masticatory performance, and overall
function.4 Moreover, well-adapted dentures may
reduce trauma to the supporting tissues and thus
minimize bone resorption, avoid the occurrence
of traumatic ulcers, and improve denture wearing
comfort, patient satisfaction, and quality of life.
Thus, the accuracy of the intaglio surface of
removable dentures is key to denture adaptation
and to a successful treatment outcome in
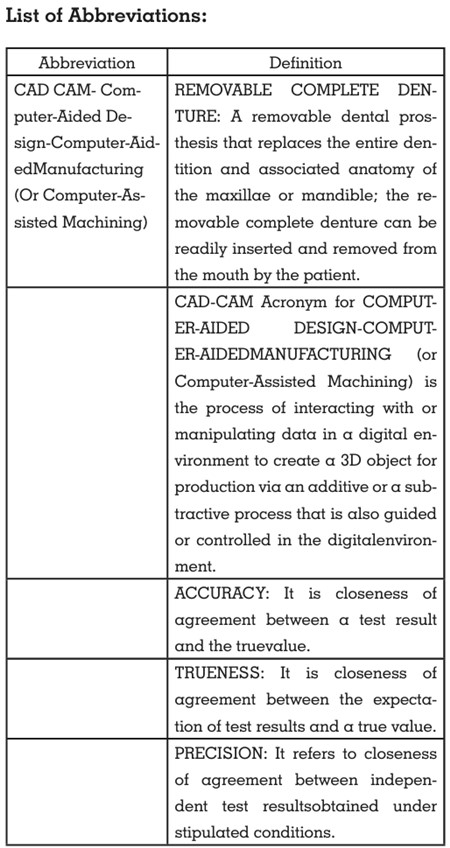
removable prosthodontics. Thus, came into
role the CAD CAM (computer-aided design
and computer-aided manufacturing) complete
dentures which were first described in 1946 and
now represent an improvement over conventional
denture production.5 There are several benefits
of the CAD CAM complete dentures including
reduced chair time, decreased number of patient
visits, simplification of the laboratory process,
produces fewer errors during the denture making
process and can allow the efficient fabrication of
a replacement prostheses i.e., duplicate dentures
based on stored data available. This is highly
helpful for elderly people who have underlying diseases and have difficulty to come to the dental
office.6 The fabrication of complete dentures by
computer-aided design and computer-aided
manufacturing (CAD-CAM) methods has gained
popularity in clinical as well as laboratory
practices.7 There are three processes involved
in the CAD/CAM workflow, the first two steps
being collection of data and CAD. The last step,
CAM process, can be done using either additive
manufacturing (three-dimensional [3D] printing)
or subtractive manufacturing (milling).2
The milling approach is a method of
fabricating dentures by removing materials
from prepolymerized PMMA (Polymethyl
methacrylate) block to form the desirable shape.
Milled dentures possess superior mechanical
qualities over conventional complete dentures
due to the absence of polymerized shrinkage
resulting in better retention.8 Milled maxillary
complete dentures have been reported to be
preferred by both dentists and patients.9 The
principal disadvantage of milling is waste
product, a lot of material remains unused from
the block and thus leads to large amounts of
wastage. Moreover, milling technique has certain
limitations such as the contour of the restoration
relies on the size of cutting tools.2 If the diameter
of the cutting tool is bigger than the diameter
of certain components, the internal fit accuracy
will be compromised, or the marginal qualities
will be degraded. Looking for alternatives that
might solve these problems we came across
3D-printing technique.10 Direct light processing
(DLP) is the most extensively used type of
3D printing in dentistry. Complete dentures
fabricated using the Rapid Prototyping(RP)
technique have also elicited patient satisfaction
comparable with that for conventional complete
dentures.11,12 The purpose of this study is to
evaluate the accuracy of the intaglio surface of the complete dentures fabricated using
subtractive and additive manufacturing. This
systematic review was conducted in accordance
with the Preferred reporting items for systematic
reviews and meta-analyses guidelines 2009 (i.e.,
the PRISMA statement).13
This systematic review was conducted according
to the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA)
guidelines13 with prior registration in PROSPERO
(Registration number CRD42023438705).
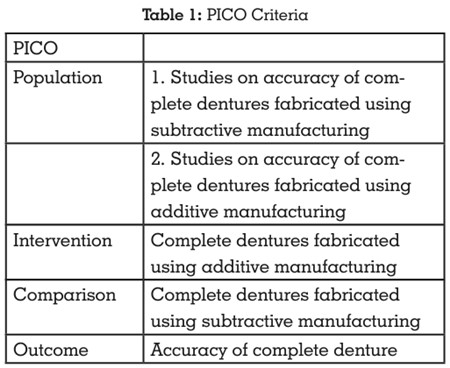
The focused question was “Is there a difference
in the accuracy of complete dentures fabricated
by subtractive manufacturing and additive
manufacturing?” The PICO i.e., the Population,
Intervention, Comparison, and Outcome format
was used (Table 1). The inclusion criteria were
studies that evaluated the accuracy of the intaglio
surfaces of the complete dentures fabricated by
additive and subtracting manufacturing methods
and articles appearing in the English dental
literature, published after year 2011 till 28th Feb
2023. The exclusion criteria were studies wherein either of the two manufacturing methods were
not considered. Review articles, case series and
case reports were also excluded.
Electronic search of PubMed (including
MEDLINE), Cochrane Central, EBSCO host
databases and Google Scholar search engine
for articles published from 1st January 2013 to
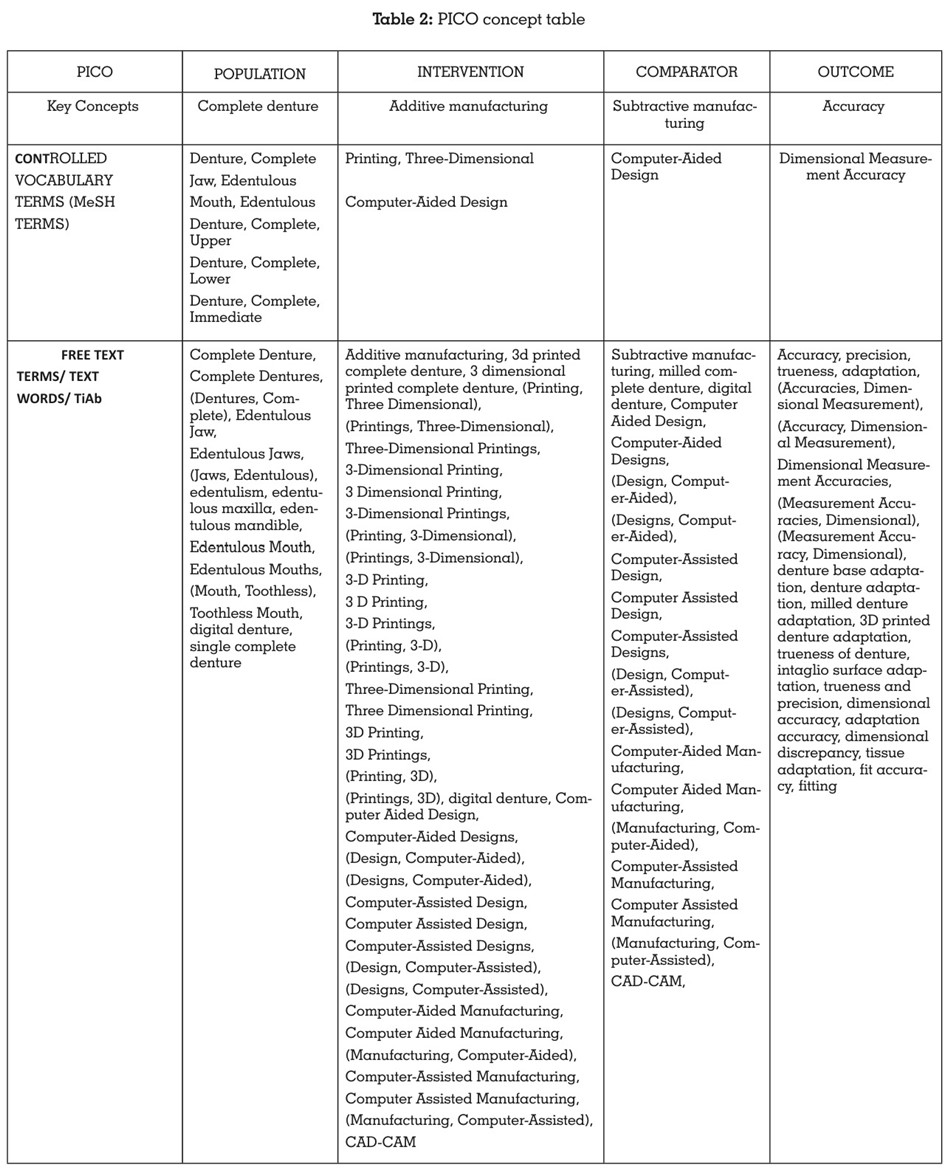
28th Feb 2023 was conducted. The controlled
vocabulary terms (i.e., MeSH terms) and free text
terms were obtained by searching key concepts
in the MeSH database and a thorough evaluation
of related articles, thesaurus, dictionaries, and
entry terms. The terms such as edentulous
jaws, edentulous mouth, edentulous patients,
fully edentulous arches, completely edentulous
arches, CAD CAM, additive manufacturing, 3D
printing, subtractive manufacturing, milling,
dimensional accuracy, trueness, precision,
surface adaptationwere combined using suitable
Boolean operators (AND, OR, NOT) (Table 2).
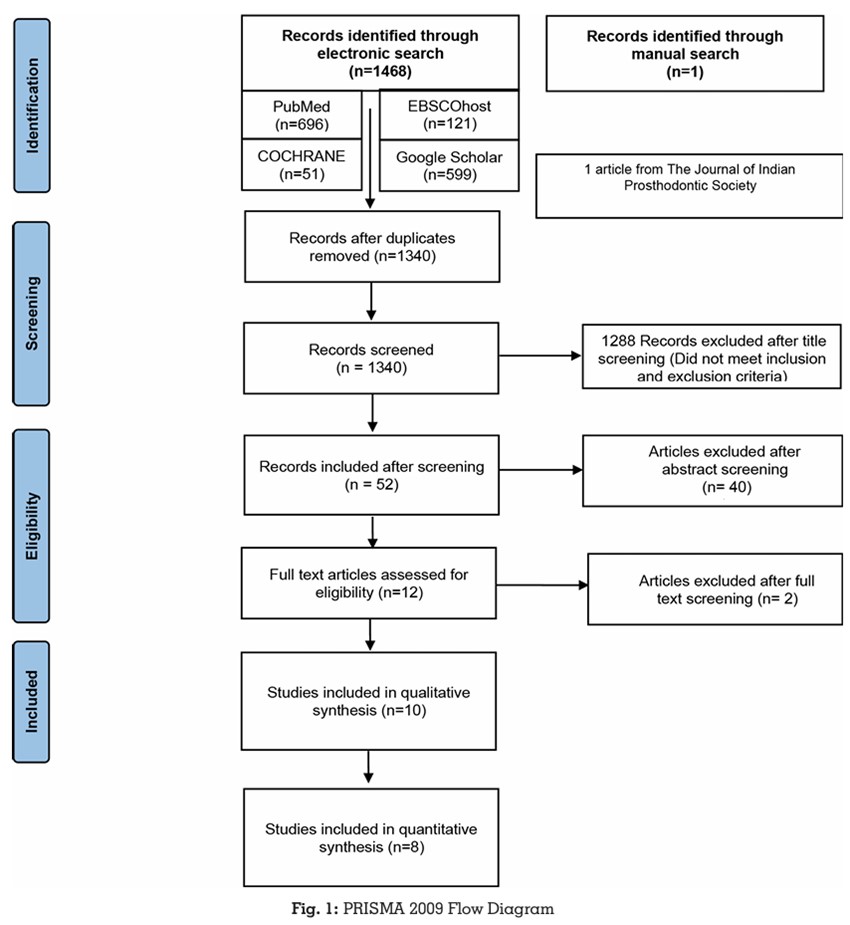
An electronic search was conducted
independently by two reviewers (D.A., S.G.)A
total of 1468 articles were obtained via electronic
search and manual search. The articles thus
obtained were evaluated for duplicates. A
detailed summary of data selection has been
put forth in the PRISMA 2009 Flow Diagram14
(Figure 1).
The study characteristics of each systematic
review were extracted including study details,
search details, analysis, and results/findings by
two independent reviewers (D.A., S.G.)
A third reviewer (P.B.) was called in for a final
decision if any disagreement persisted between
the two calibrated reviewers.
The 1467 articles that were obtained through the electronic searches were compared
meticulously with respect to the author’s name,
year of publication, title, abstract as well as the
journal name, issue, and volume number. The
articles thus obtained after the electronic and
manual searches, were evaluated for duplicates
using the Mendeley Desktop software (v1.19.6).
The 1 article obtained through the manual
search was added manually using the ‘add entry manually’ feature of Mendeley Desktop
software (v1.19.6). The ‘check for duplicates’
feature of this software was then used to identify
and eliminate duplicates. 128 duplicate articles
were identified and subsequently eliminated
leaving behind 1340 articles. Two calibrated
reviewers (D.A, S.G.) independently screened
the relevant titles of the studies found through
the electronic search. Out of 1340 articles, 1288 articles were excluded after screening of the
title. The articles thus eliminated were either
literature reviews, scoping reviews, case reports,
case series, or articles not utilising additive or
subtractive manufacturing for complete denture
fabrication. Thus, 52 articles were selected after
title screening.
Two calibrated reviewers (D.A, S.G.)now
independently screened the abstracts of the
studies found relevant during the screening of
the titles and a total of 40 articles were further
excluded after abstract screening. The articles
eliminated through abstract screening were
mainly involving different manufacturing
methods for the dentures. 12 articles were
included after abstract screening. Out of the 12
articles, 10 met the inclusion criteria and thus were included in this systematic review. Out of
all the included studies, 8 were invitro studies
and 2 were clinical trials.
A third reviewer (P.B.) was called in for a final
decision, if any disagreement over article
selection persisted between the two calibrated
reviewers. Inter-reviewer reliability was checked
via Cohen’s kappa coefficient.15 The Cohen’s
kappa coefficient values obtained for title,
abstract and full text screening was 0.62, 0.68
and 0.75 respectively, indicating moderate inter
reviewer agreement for title, abstract and full
text screening.
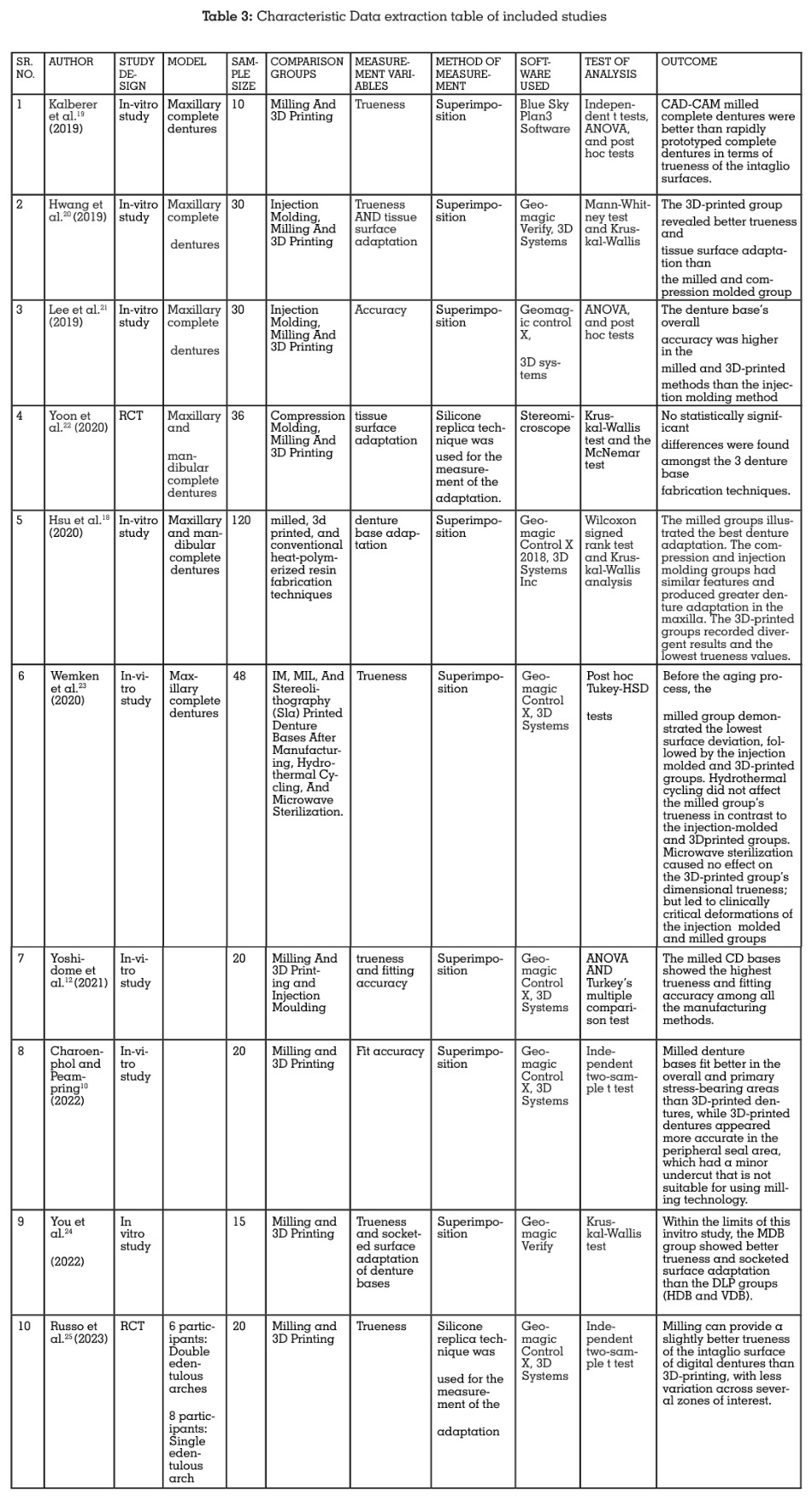
The data was subsequently extracted from the
10 included studies and recorded in 2 excel data
extraction sheets as mentioned in the summary table (Table 3).
The data extracted was entered under the
following headings: Author and Year of
publication, Study design, Study model, Sample
Size, Comparison groups, Measurement
variables, Method of measurement, Software
used, Test of Analysis, Outcome.
Risk of bias assessment of the included studies
was done using the QUIN tool scale16 for in vitro
studies and The Cochrane Collaboration’s tool17
for Randomized controlled trials for RCTs by two
independent reviewers (S.G., D.A.).
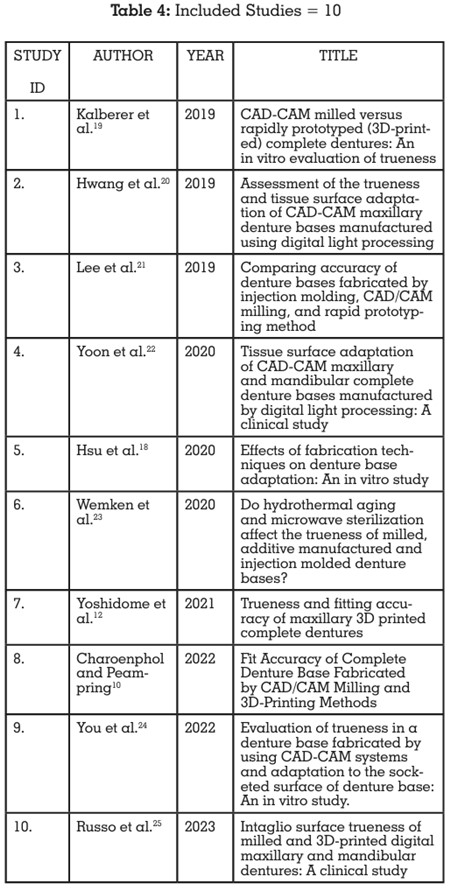
Out of the 10 studies, 8 included studies were
in-vitro studies, hence the Quin tool scale was
considered apt for the risk of bias evaluation
for them in this systematic review. The changes
made to the scale were validated by the third
reviewer (P.B.) (Table 4).
The risk of bias of all the 8 included in vitro
studies ranged from 79% to 87%, which falls
under the category of low risk of bias.
For the 2 excluded clinical studies, The Cochrane
Collaboration’s tool was considered apt (Table
5).

The changes made to the scale were validated
by the third reviewer (P.B.)
10 studies evaluating the accuracy of digital
complete dentures fabricated either by additive
manufacturing or subtractive manufacturing
were included in the systematic review.
Two studies which compared the accuracy of
the intaglio surface of the complete dentures
fabricated either by milling or by 3D printing
(Hsu et al. 2020 and Yoshidome et al. 2021)12,18
were excluded from meta-analysis due to lack of
data availability in terms of mean and standard
deviation values respectively. The eight studies
which evaluated the intaglio surfaces of the
complete dentures fabricated by additive and
subtractive manufacturing (Kalberer et al. 2019,
Hwang et al. 2019, Lee et al. 2019, Yoon et al.
2020, Wemken et al. 2020, Charoenphol and
Peampring 2022, You et al. 2022, Russo et al.
2023)10,19-25 were included for meta-analysis.
The Review Manager software (Version 5.4.1)
was used to perform meta-analysis. Mean
values and standard deviations for accuracy
by assessing surface deviation of dentures
fabricated by milling and 3D printing were
included for the analysis.
The primary outcome measures the accuracy of
the intaglio surface of the complete dentures. The
data was tabulated under the headings of study
name, group, and effect size. The effect size was
calculated on the continuous raw data entered
for mean, standard deviation, and sample size.
95% confidence interval for each effect size was
also computed. The heterogeneity of effects was assessed by the Higgin’s I2 test.26,27 The I2
statistic describes the percentage of variation
across studies that is due to heterogeneity rather
than chance and is denoted by the formula:
I2= 100% x (Q-df)/Q. According to Higgins et
al, calculation of heterogeneity is essential in
determining the generalizability of the findings
of meta-analysis.27
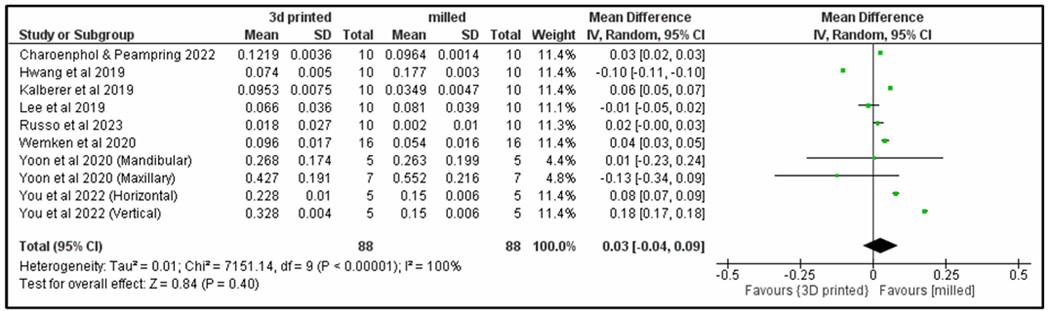
The result of the meta-analysis for accuracy
of CAD CAM complete dentures showed less
surface deviation in milled complete dentures
(subtractive manufacturing) when compared
to 3D printed complete dentures (additive
manufacturing). (Figure 2)
The advent of computer aided designing and
computer aided manufacturing (CAD CAM)
technology has paved the way for a highly precise
and efficient digital work flow.28 There are three
processes involved in the CAD/CAM workflow.
The first two steps in the process are collection of
data and CAM. The last step, CAM process, can
be done using either additive manufacturing
(three-dimensional [3D] printing) or subtractive
manufacturing (milling).29 These two methods
have been considered in this systematic review.
This systematic review has segregated the
accuracy achieved on using additive and
subtractive methods for manufacturing complete
dentures. The two techniques used to assess the
accuracy were superimposition technique for
studies where scanning was performed to attain
impressions and the silicon replica technique
in situations where manual impressions were
made.
Amongst the articles included in this systematic
review, Kalberer et al19 (2019) concluded that
milled complete dentures, under the present
manufacturing standards, were superior to the 3D
printed complete dentures in terms of trueness of
the intaglio surfaces. However, further research
is needed on the biomechanical, clinical, and
patient-centered outcome measures to determine
the true superiority of one technique over the
other about fabricating complete dentures by
CAD-CAM techniques. Hwang et al20 (2019)
conducted an in vitro study and stated that the
3D printed maxillary denture base showed better
trueness and tissue surface adaptation than the
milled and pressed denture bases. The printed
denture bases reproduced the morphologic
irregularity of the residual ridge, while the
milled denture bases had minor inaccuracies.
However, the study design was in vitro and
therefore more clinical evidence is required to
draw any conclusion. Lee et al21 (2019) and Yoon
et al22 (2020) addressed that both 3D printed and
milled denture bases were likely to show intimate
adaptation compared with other techniques.
Both the studies showed no significant
differences amongst both the groups. Hsu et
al18(2020) concluded that the milling technique
had the best denture adaptation, whether
using the silicone thickness measurement
or digital superimposition analysis. Milling
technique improves the adaptation whether for
maxillary or mandibular denture bases, but the
printing technique presents divergent accuracy. Wemken et al23 (2020) concluded that subtractive
manufacturing of denture bases results in the
highest trueness, followed by injection moulding
and 3D printing. The author also subjected the
dentures to hydrothermal cycling and microwave
sterilization. In contrast to injection moulding
and 3D printing, hydrothermal cycling did not
affect milled denture bases. However solely SLA
printed denture bases remained dimensionally
stable after microwave sterilization. In a clinical
study conducted by Russo et al25 (2023), within
the limits of the manufacturing methodologies
used for complete dentures, milling provided
better trueness of the intaglio surface when
compared to 3D printed dentures. The in vitro
studies conducted by Yoshidome et al12 (2021),
Charoenphol and Peampring10 (2022) and You
et al24 (2022) concluded that milled complete
denture bases showed the highest trueness and
fitting accuracy among all the manufacturing
methods. Thus, a systematic review compiling the
conclusions of these in vitro and clinical studies
was conducted to draw a conclusion regarding
the improved accuracy of complete dentures
when fabricated by different methodologies i.e.,
additive, and subtractive manufacturing.
The Quin tool16 for invitro studies and Cochrane
tool17 for RCTs has been used to identify the risk
of bias of the individual studies.
Eight out of the 10 included studies seemed to be
relatively homogenous in their study design and
outcome variables. Hence, a quantitative analysis
by means of a meta-analysis was planned. Meta
analysis is a systematic procedure for assessing
and combining statistical information based
on results of available independent studies
regarding the same topic.30 The results of the
quantitative analysis have been provided in the
form of forest plots for easy visualization.
The heterogeneity of the primary studies has been evaluated using the Higgins’s I2 test.11
Heterogeneity refers to differences in results
between primary studies that are greater than
expected by chance alone.
The result of the meta-analysis for accuracy
based on surface deviation showed less accuracy
for 3D printed dentures compared to the milled
complete dentures.
Limitations of this systematic review were; The
search for this study was limited to articles
published in the English language. Also, grey
literature has not been searched for relevant
literature. This could have resulted in mild
selection bias.
The results of this systematic review should be
applied with caution to the clinical scenario
since most of the included studies are in-vitro in
their study design.
Within the limitations of this systematic review and meta-analysis, the following conclusions could be drawn: